For the best part of a year, Kiwis were urged to get vaccinated to protect their families. However, this week’s concession that Pfizer never tested the vaccine to confirm whether the vaccine prevented transmission, has rocked the European Parliament.
Pfizer executive Janine Small admitted that the company didn’t have data on whether the mRNA gene technology prevented transmission of infection. In a tweet, a Member of the European Parliament said ‘this is scandalous’.
And no, the clinical trial data never included prevention of transmission of infection as an endpoint.
This is one more step for public understanding regarding how information and science has been ‘managed’ during 2020-22 in order to shepherd the public to accept a novel technology; a high-risk biological entity.
It appears that the New Zealand government knew all along. The traffic light system used during the pandemic ‘was never designed to dampen down transmission, it was only designed to nudge people towards vaccination’.
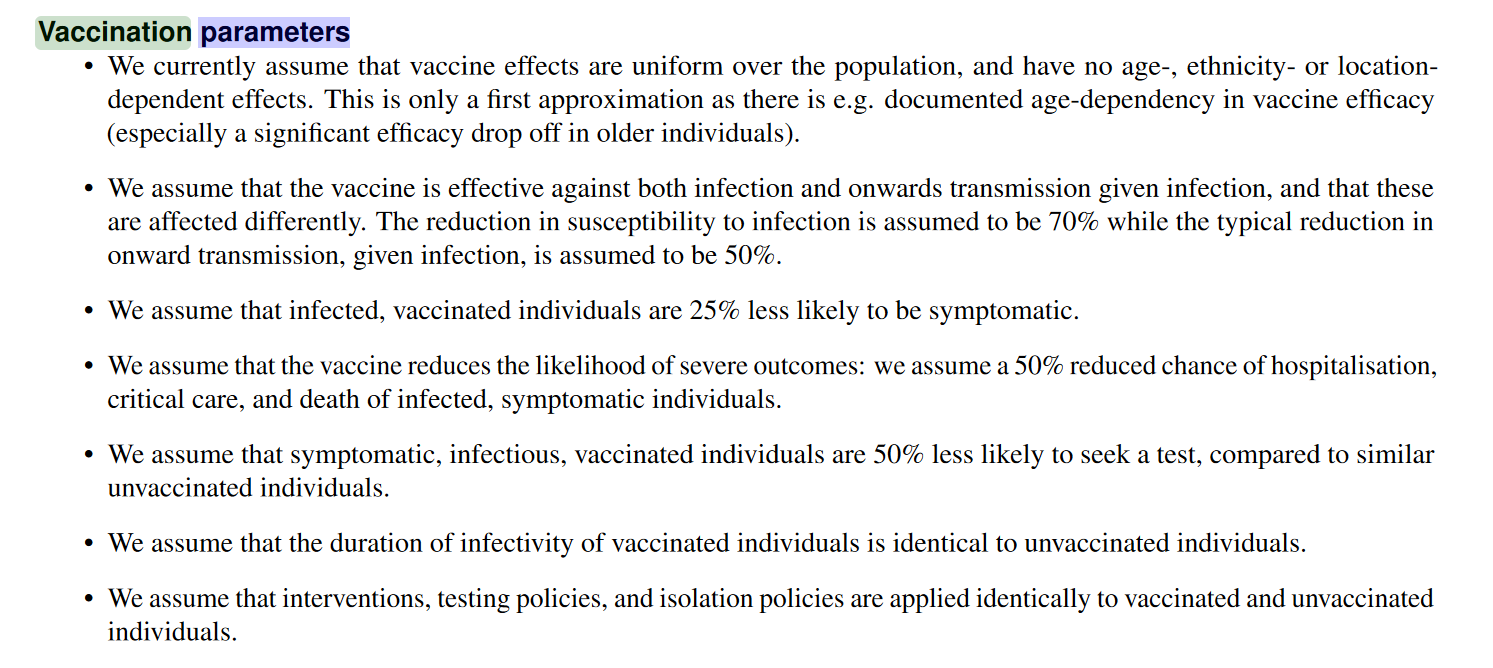
Modelling that claimed traffic light systems would reduce transmission of infection, was based on assumptions rather than hard data.
Most of us looking at the trial endpoints and the science have known this. But the public didn’t.
This paper has not yet undergone external peer review Estimates of effects on changing Alert Levels for the August 2021 outbreak
The mRNA technology was made broadly available to the general New Zealand public in the second half of 2021. Most Kiwis thought that vaccination would protect prevent, or demonstrably limit the passing on of the SARS-CoV-2 virus.
By October 2020 it was clear that risk of hospitalisation and death from infection was stratified to the elderly and to those with multiple health conditions. Eminent epidemiologist Professor John Ioannidis published a paper that clearly stated that risk ranged widely – with ‘over 1,000-fold variability between children and elderly nursing home residents.’
Despite this, healthy people were compelled, through force of law, to accept the injection or suffer a range of extreme financial and social punishments. The mandate rationale was about protecting others.
New Zealand businesses were advised:
‘Studies show that about 95 per cent of people who have received both doses of the vaccine are protected against getting COVID-19 symptoms. This means that once you are fully vaccinated, you are far less likely to fall seriously ill and less likely to transmit the virus to friends, whānau or workmates.’
The 95 per cent claim was based on vaccine efficacy 7 days after the second dose. There was no data on prevention of transmission, which might include healthy asymptomatic populations.
Our Ministry of Health, advises Kiwis that the vaccine will ‘help prevent you from getting infected’ – but there’s still no data confirming this. The clinical trials never included seroprevalence tests and seroprevalence data seemed outside of the remit of the New Zealand government.
The mRNA technology was never a traditional vaccine. It contained instructions to reproduce an antigen, the inflammatory spike protein in the body. Immediately after release significant adverse events were reported. It was not sterile, and papers were constantly published demonstrating waning, breakthrough events, and high viral loads in vaccinated populations.
The only problem is, the New Zealand government’s primary ‘evidence’ for policy came from the clinical trial data and regulatory reporting. Raw data often hides unfavourable content. For example, there was four-times the cardiac arrests leading to death in the vaccinated group. In addition, adverse events are famously under-reported.
In government policy papers we see heavy regulatory reliance and cherry-picking of studies to justify policy. There’s a failure to address the fact that healthy groups weren’t at risk of hospitalisation and death – instead they were at risk of higher vaccine-related events.
The Ministry of Health Chief Science Advisor Ian Towns’ justification for childhood (5-11-year-old) vaccination relied on outdated science to identify numbers needed to treat, and primarily focused on industry-friendly data to consider vaccine-related harm. Town’s December 2021 paper could have widely reviewed the literature. It could have looked at absolute risk, but it didn’t.
Government evidence weighted towards protected data supplied by the Pfizer corporation. The approval was primarily based on the data from Study C4591001 which confirmed symptom suppression at two weeks. This continued, throughout the pandemic, to be ground zero for reasoning for approval of the novel gene therapy.
Nowhere at all – was the approval based on the prevention of transmission of infection.
Many of us have attempted to find out through Official Information Act requests, where the work was being undertaken to survey the scientific literature to understand the state of science.
But we’ve been dismissed and ignored when we’ve tried to understand safety and efficacy by age and health status. The government never did this work.
A massive complex legislative process designed to keep the public placated, but excluded from any consultation, ensured vaccine mandate legislation was unimpeded.
Covid legislation was overseen by the Minister for COVID-19 Response. Until June 2022, the Minister was the Hon Chris Hipkins.
Mandates legislation were predominantly made as Orders. Orders were made under section 11 of the COVID-19 Public Health Response Act 2020 in accordance with section 9 of that Act. Production was prolific. Orders are secondary legislation, outside of Parliamentary consideration, and outside democratic scrutiny, with all the power of primary legislation.
In October 2021, the public were given a brief chance to comment on an amendment to the COVID-19 Response Act. As myself and colleagues from Physicians and Scientists for Global Responsibility, (a charity with a twenty-year history of drawing attention to science, technology, and regulation), noted in our submission, by October it was evident that the vaccine waned and that breakthrough infections were common.
In an oral presentation to New Zealand Members of Parliament, before the mandates rolled out, we implored MPs including Dr Liz Craig not to take stricter measures around vaccination.
Chris Hipkins was in charge of the COVID-19 Public Health Response Amendment Bill (No 2). However, because vaccines weren’t a focus of the Bill, the 14,000 members of the public who submitted were largely out of scope.
When the public were submitting in October, Hipkins was overseeing the production of parallel legislation. The COVID-19 Public Health Response (Vaccinations) Order 2021 only mentioned vaccines 102 times. By the time the separate Amendment Bill was passed on November 20, this other Order referred to vaccines 299 times.
While public comment ended on October 11, on October 25, Chris Hipkins extended mandates to:
‘Workers over the age of 12 years who carry out work at or for an affected education service (including as a volunteer or an unpaid worker)’ including home-based education and care service.’
The power for this came from new iterations of the parallel Orders.
Then, on Saturday November 23, Hipkins’ next job, the COVID-19 Response (Vaccinations) Legislation Bill 2021, was rushed through Parliament in one day. There were no impact statements in the Bills Digest. The terms vaccine/vaccination were mentioned 155 times. (Counting the amount of times a term is referenced can draw attention to the weight of an issue in discourse or rhetoric).
The Amendment Bill had received Royal Assent three days prior.
Once this Bill was passed – the COVID-19 Public Health Response Act was updated to incorporate these changes. Therefore, while the November 20 version of the Act, (after public consultation) vaccines weren’t mentioned at all – by the November 26 version, vaccines were well bedded in.
The public had been largely excluded from any policy process or discussion which involved vaccination policy.
The November 26 version was the legislative instrument that locked in the requirement for a vaccination certificate to be presented for access to premises, resources, and activities.
The unvaccinated missed out on trips to national parks, hairdressers, church, and sports. They couldn’t get their drivers licence, sit down for a coffee, or attend the gym. They were outcast.
Twelve-year-olds couldn’t swim, or play rugby or tennis or badminton if they weren’t injected.
Over this period – it was the Minister for COVID-19 Response, the Hon Chris Hipkins, who decided that this legislation should be produced and released.
However, we are yet to see any material that demonstrates the methods by which the risk was weighted. How did he decide on legislation which necessitated such unprecedented, hard-line measures? It is an open question.
The Hon Chris Hipkins, as standard practice, boots all Official Information Act Requests to the current Minister for COVID-19 Response, Ayesha Verrall.
I’ve complained to the Ombudsman, only to find that the Hon Chris Hipkins is exempt from the Official Information Act requests relating to COVID-19 because he switched portfolios. The Minister for Police doesn’t have to answer questions from when he was Minister for COVID-19.
Data modelling created the justification for the roll-out of pandemic technology. However, this relied on values established earlier on in the pandemic, before Omicron was the predominant strain. The public never knew that while children and young people contract and pass on the infection more quickly, this group was not only at low risk of hospitalisation and death from Covid – but that post-infection this group produced a natural immunity buffer. This group would make it harder for future variants to gain hold.
For the second half of 2021, the public knowledge and advice to under 40-year-olds concerning the risk of pericarditis/myocarditis was effectively suppressed. Myocarditis risk was well established by November 2021.
Informed consent was impossible, as doctors who recommended that healthy patients not get the vaccine were reported on, and had their medical licence suspended.
In New Zealand in December, with the traffic system in place, young people were urged to just ‘get the jab done’.
In October 2022, doctors remain under gag orders. In California, it is illegal for doctors to disagree with the current government opinion on Covid. Medical councils in New Zealand and Australia have come down hard on doctors who dissent from the central government position.
In addition, even though Pfizer acknowledged that immunosuppressed groups with multiple health conditions might be at risk of vaccine failure – from the earliest months of 2020, the New Zealand government effectively prohibited the use of early treatments. Early treatments were designed to prevent the cascade of symptoms that the elderly and multimorbid were most at risk of. The recommended drugs had a long history of safe use. The government never transparently reviewed their position. Early treatments in New Zealand are rudimentary in comparison to those recommended by international groups of medical doctors.
Meanwhile, bad news on boosters and their relatively short period of efficacy continues to be released.
A pandemic is a dynamic, living thing. Weekly and monthly, risk changes as variants mutate, as the gene therapy technology became both more outdated and more widely studied, as researchers and scientists gained greater clarity on who was most at risk, and why they are at risk.
We have in front of us, a chilling precedent for future pandemic event responses. The global pandemic response was predicated on global injection of a novel therapy, based on data supplied by the manufacturer, who has subsequently quadrupled their revenue in 2021 and 2022. It was based on advice from the World Health Organisation, who is deeply reliant on funding from individuals and companies involved in vaccine manufacturing.
Right now, the public can submit to the ‘Ethical Guidance for a Pandemic’ consultation. The proposed guidance fails to look at the fails – the mangling of science, and the privileging of private industry data. The document refers to Covid hundreds of times, but fails to acknowledge want went wrong.
The guidance document ups the ante on technological surveillance, and policies that steer towards compliance for vaccination. It continues the government ideological failure to link diet-driven disease with pandemic risk and fails to address the inequities that drive chronic and immunological health risk.
It profoundly ignores the fact that the generally healthy should not be subject to policies that restrict human rights and potentially harm health.
The scandal may be perpetuated in future, if science continues to be shaped and shepherded for narrow ends, while broader obligations to protect overall health are downplayed and dismissed.
Jodie Bruning is a New Zealand based sociologist and is a trustee of Physicians & Scientists for Global Responsibility (PSGR.org.nz). Papers and writing can be found at Brownstone Institute, TalkingRisk.NZ and at JRBruning.Substack.com and at Talking Risk on Rumble.